This November, the distinguished American Society of Addiction Medicine (ASAM) will release the Fourth Edition of The ASAM Criteria, which sets the standard for clinical care in addiction recovery. Guidelines for placement, continued stay, transfer, or discharge are followed by behavioral health programs to ensure quality care. The latest release has been informed and vetted by diverse stakeholders in response to the developing needs of the healthcare field. As a result, the updated standards for treatment help care managers make better, more objective decisions based on the established guiding principles.
The updated continuum of care promotes:
A CHRONIC CARE MODEL - Ongoing care for those in remission.
INTEGRATION OF CARE - Incorporating biomedical and psychosocial services for withdrawal management and continued care for clients with acute biomedical concerns.
CO-OCCURING CAPABLE CARE - Integrated care for mental health conditions.
ACCESS TO RECOVERY SUPPORT SERVICES - Coordination between addiction treatment programs and recovery residences.
HARM REDUCTION - More patient involvement in goal setting, preferences, and access to addiction medication.
The Fourth Edition offers operating standards for the Level of Care Assessment (used to determine the recommended level of care) and the Treatment Planning Assessment (used to develop the comprehensive treatment plan.) Each multidimensional assessment must consider biological, psychological, social, and cultural contexts. A thorough evaluation of problems and strengths is vital to developing a successful, patient-centered treatment plan.
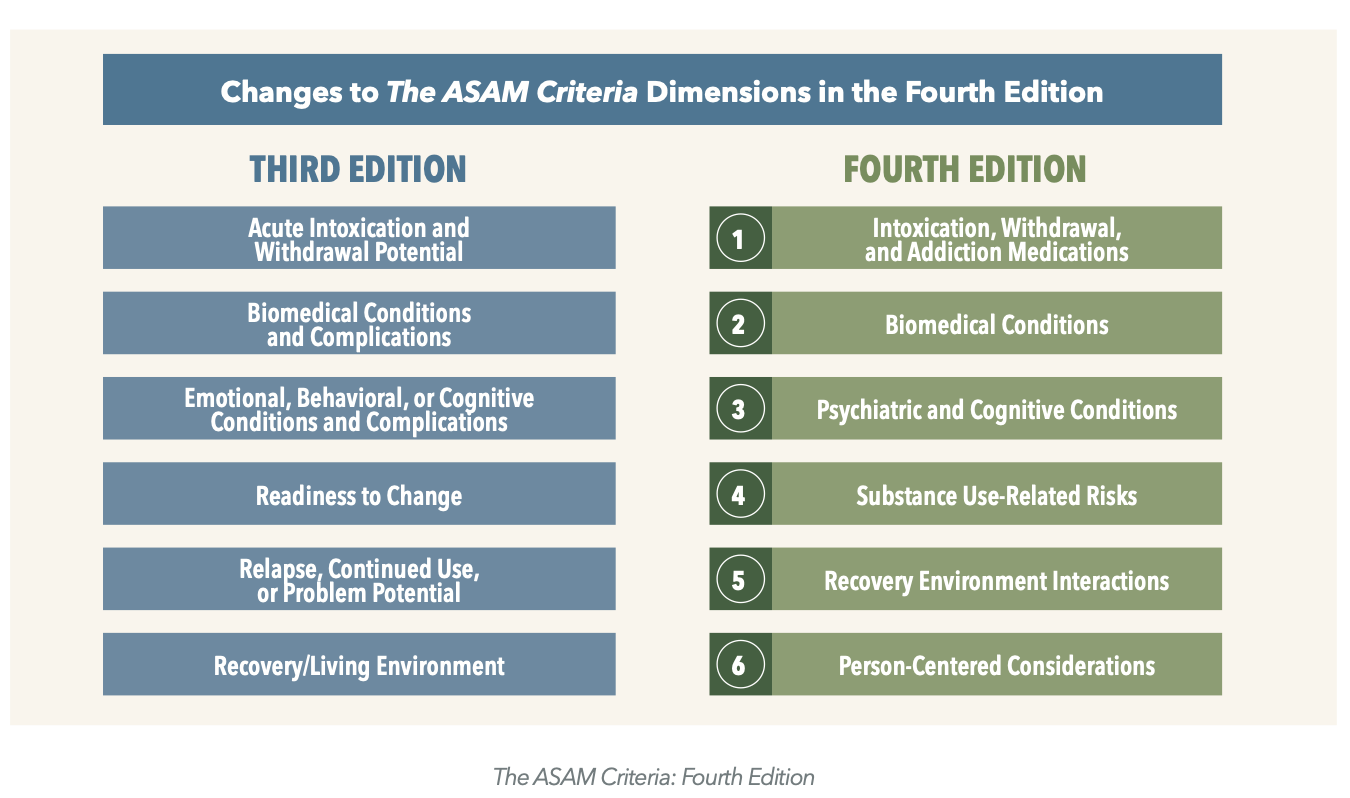
The ASAM Criteria Dimensions updates make it easier to understand and share these standards while keeping up with the changing terminology in the field. The subdimensions introduced will help the clinician make recommendations based on their findings and the patient's willingness to engage.
Integrating Trauma-Sensitive Practices, Culturally Humble Care, and Social Determinants of Health
Addressing Pain
Addressing Cognitive Impairment
The behavioral health programs that adopt these standards and track their metrics are more equipped to provide evidence-based care for their clients. A task-based workflow that charts progress and automates documentation improves outcomes. Alleva’s data-driven EMR helps optimize and streamline the standards compliance process. Compiling outcome data with our advanced business intelligence tools and built-in task-based documentation options helps reduce error and burnout.
If you want to learn how Alleva’s state-of-the-art EMR platform can upgrade your program to meet the highest standards of care, book a quick, hassle-free demo tailored to your needs.
After beating the odds and conquering the demons of addiction, why would anybody voluntarily choose to return to their previous self-destructive state? It is not uncommon for those in recovery to experience sobriety for a long period of time, and on an impulse restart the self-destructive cycle. This is what we call relapse.
Although the behavior may seem inexplicable, understanding brain chemistry sheds some light on the situation. Because the effects of drugs are so powerful, it changes the brain structure and chemistry of the user. Prolonged usage of such addictive substances leads to a reprioritization of what the brain ranks as important. With time the addict’s brain can even prioritize the use of the drug above natural survival responses such as eating and sleeping. The addict’s brain convinces itself that the consumption of the drug is more important than their life.
Our survival responses are powerful, to say the least. We are hard-wired to do whatever it takes to ensure the preservation of our lives. I once witnessed a mouse stuck in a trap chew off its own arm to escape. Just like the mouse, any of us would go to undeniably extreme measures to survive in a life-threatening situation.
Because of the effects of reprioritization, addicts will go to similarly extreme measures to ensure they can continue the usage of their substance. In short, addiction knows no limits. There is no price too expensive, no situation too dangerous, and no risk too great. Even after enjoying years of sobriety, there is still a danger of relapse. This is why addiction treatment must extend beyond the sphere of treatment centers. Truly, quitting the use of the drug is just the first step.
Behavioral Health facilities using Alleva's telehealth feature are able to reach thousands of isolated clients in despair using their built-in Zoom Video technology.
LAGUNA NIGUEL, Calif. (PRWEB) May 20, 2022-- In the wake of COVID-19, the U.S. not only faces a devastating death toll of over 980,000 lives lost from the virus but a staggering number of over 100,000 additional “deaths of despair” from alcohol abuse, drug overdoses, and suicide. This is a 28.5% increase in overdose cases from before the pandemic. With the burden on behavioral health facilities continuing to build, Alleva teamed up with Zoom Video Communications, Inc. in 2017 to offer a comprehensive telehealth solution that enables behavioral healthcare companies to meet HIPAA compliance requirements while delivering exceptional care.
Even before the pandemic, Alleva recognized the utility of Zoom’s unified communications platform and its application for healthcare facilities. Since its implementation, clinicians have been able to stay in contact with their clients who are unable to attend in-person sessions and those who prefer remote treatment. Before Covid, Alleva's customers averaged around 60 thousand telehealth minutes a month, but in April of 2020, and the onset of pandemic restrictions, that number jumped to almost 2 million minutes a month. Even as Covid risks have diminished, telehealth has not tapered off.
“The demand for telehealth shows no signs of slowing,” said Paul Magnaghi, Global ISV Program Leader, Zoom. “It’s crucial to provide a simple, frictionless, and secure experience for everyone involved–from provider to patient. Our platform incorporates security controls to help enable customers to satisfy the HIPAA Security Rule. We are pleased to have Alleva join Zoom’s ISV Partner Program and provide a simple and quick way for people to get connected to the care they need.” With the integration of Zoom’s convenient technology and the Alleva EMR, treatment centers can sync calendar appointments, and send invitations and reminders via texts directly to the Alleva app on their client’s cellphone, all while enabling HIPPA compliance.
Steven McCall, CEO of Alleva, said, "The fact that we were among the first EMR platforms to add the telehealth feature back in 2017 meant that we were agile and responsive when clinicians' circumstances and needs changed. Alleva is all about offering the latest technology and making life easier for caregivers.”
Alleva’s telehealth feature has allowed substance abuse and behavioral specialists to connect to their clients during increasingly challenging times. With options for individual, group, family, and admissions sessions, the telehealth feature allows people to connect effortlessly through digital means, with room for continued innovation. Moving forward, Alleva is looking to expand their solutions to further streamline communication and connect substance abuse specialists to those who need it.
For more information about Alleva, its built-in telehealth solutions, and how its solutions are shaping the behavioral healthcare industry, visit HelloAlleva.com.
About Alleva
Alleva provides world-class software to the behavioral health industry. Made up of a team of licensed therapists, industry professionals, and experienced software developers, they seek to use their industry background and passion to help the helpers give better care by providing them with supportive technology.
It has long been a challenge for those in the substance abuse and mental health professions to get their clients to engage in treatment in the time between sessions, or for those in a residential facility, to keep them on the right track after discharge. Especially in the wake of COVID-19, clinicians are searching for ways to help their clients seek and access the resources available to them at home.
While on some levels, technology can seem to lead us to disconnect from others in favor of virtual versions of ourselves, it also presents us with innumerable supportive resources to assist clients with taking ownership of the recovery process, while dedicating time and attention to caring for themselves on a mental, emotional, and physical level.
The following is a summary of four types of apps that can be helpful resources for your clients, while in therapy and long after.
Meditation Apps
Mindfulness and meditation are taught in therapy as a means of connecting clients to internal resources to harness healing outside of the session.
An integral part of meditation is eliminating and/or directing awareness away from distractions. Meditation apps do this wonderfully by changing technology from a distraction into a tool. By facilitating meditation practices and activities, meditation apps also increase the self-efficacy of clients and confidence in their mental awareness.
Insight Timer- Insight Timer offers the unique experience of several forms of guided meditations for various needs. Music, guided imagery, and muscle relaxation are some of the few forms of meditations available on the app.
10 Percent Happier- 10 Percent Happier is a wonderful app for those who are new to mediation. Courses and coaches set this app apart from more independent meditation apps.
Reading Apps
Bibliotherapy refers to the use of literature in the healing process of counseling or therapy. Some therapists prefer to assign materials for clients to read based on treatment goals. However, some may encourage clients to simply explore as they feel comfortable, as for the ever-anxious, picking up a fantasy fiction novel may be the perfect distraction to get them out of their heads for a while.
In addition to Audible or Kindle, consider some additional reading apps for use in your therapeutic process:
OverDrive- The OverDrive app offers app users the chance to connect with local libraries in order to browse and read any of the volumes available nearby, in addition to the books on file with OverDrive.
Nook app- The Nook reading app from Barnes & Noble offers a large selection of literature spanning multiple genres.
Sleep Apps
Research on sleep hygiene and its connection to mental health and wellness is growing rapidly. In fact, a routine question in mental health services intakes is: “how many hours of sleep do you get on average?”
Sleep apps are available to promote proper sleep hygiene by helping clients set alarms for sleep and wake times, tracking REM (deep sleep) cycles, noting restless periods of sleep, prompting appropriate times to turn off lights and technology, and offering music to assist with falling asleep.
The following are a few sleep apps available to assist you with establishing and maintaining important sleep hygiene habits:
Slumber- The Slumber app uses both meditations and music to assist app users to attain restful sleep. Some of the “techniques” available on the app include: “mindfulness, breath control, guided imagery, and progressive muscle relaxation.”
Sleep Cycle- The Sleep Cycle app is an innovative app created to tailor the morning alarm to your stages of sleep. The app maintains a record of your sleep cycles and uses this information to wake you in the lightest stage of sleep. Thus you’ll wake feeling rested, rather than the alternative where you’re abruptly pulled from a deep sleep.
Time Management Apps
Depending on the presenting concerns of clients, time management may be a targeted skill in therapy. While this may not appear to be a primary issue, learning and embracing effective time management can contribute to reduced stress and anxiety.
Counselors and clients alike find it helpful to tackle some of the practical issues with daily life before diving deeper into the therapeutic process. Time management apps, much like personal assistants, are available to provide a central place to track the important events and tasks in life while allotting time for self-care.
Below are a few current time management apps to assist with organizing and following through with life tasks to promote healthy efficiency:
MyLifeOrganized- My Life Organized is a time management platform offering users tools for prioritizing tasks in a daily planner and various formats. This app encourages optimizing your time by helping you manage the tasks entered and organized in the app.
Remember The Milk-Remember the Milk is an application designed to help keep track of the tasks and appointments in life that may slip by. This app is designed to “get to-dos out of your head” to reduce stress and increase concentration on the tasks you want to prioritize.
An App for You: Alleva
After helping your clients find and access apps that are supportive of their recovery, try one of your own: Introducing Alleva, the friendliest EMR platform around. Alleva not only has a client app meant to keep clients connected during and aftercare, but you will also be able to easily send out text surveys and have access to the latest in telehealth technology.
Speaking of time-management skills, Alleva’s built-in, real-time alerts will also remind staff to dot I's and cross T's to ensure compliance. Alleva is the perfect example of harnessing technology that allows you to spend more time where your heart is -serving those in your care. Request a demo today.
What is HL7? It stands for Health Level-7 and is a set of international standards, rules, and definitions used to exchange and transfer medical information between health care providers. This is commonly done through electronic health records (EHRs). It's called level 7 because it focuses on the application layer, also referred to as layer 7.
HL7 has a structure for exchanging and sharing health care information electronically. Its standards set in place how that information is exchanged between health care providers and that includes the language, data type, and structure.
What are HL7 standards?
Standards for HL7 have been grouped into seven different sections. Here's a synopsis of each section for you:
Primary standards: These are the most common/popular standards. You can learn more about the specific primary standards here. Keep in mind that these are the most frequently used for system integration and compliance. So, it's a good place to start.
Foundational Standards: These are the basic tools or fundamentals the standards were built on and the technology that you as a medical professional implementing HL7 standards has to manage.
Clinical and Administrative Domains: This is where you will find standards on HL7 documents and messaging. Typically, you will have primary and foundational standards in place before getting into standards for clinical specialty standards.
EHR Profiles: The standards for EHRs make it possible for you to build an electronic health record system with models and profiles. If you're looking for a new EHR, here's a blog post on how to choose an EHR. It deals specifically with how to choose a behavioral health EHR but the principles apply to all EHRs.
Implementation Guides: This section helps you implement and support documents that were made for the purpose of a current standard. Each document here will be used as supportive material for one of the other standards.
Rules and References: These are the programming structures and guidelines for the growth and expansion of standards and software.
Education and Awareness: In this section, you'll find the Standards for Trial Use (STU) and other projects currently happening. There are also various tools and resources here to help you understand HL7 and put it into practice.
HL7 Messages
A lot of questions dealing with HL7 revolve around HL7 messages. So I want to answer a few of these questions for you. Some of these include "what is an HL7 message," "how are HL7 messages transmitted," and "what are HL7 message types?" I'll answer these questions to help you get a better understanding.
What is an HL7 message?
The whole point of HL7 messages is to transfer data electronically between various health care providers. These messages are sent whenever events happen with patients, such as when you admit a patient into your clinic. These messages are comprised of segments in a specific sequence. However, these segments are sometimes optional, sometimes required, and sometimes they're repeatable.
Message Types
Message types are present in every HL7 message as they explain why you're sending the message in the first place. Each message type has a specific code of three characters and they trigger an event. Now you're probably wondering what a trigger event is. Simply put, it's an actual, real-life event that sparks the communication needed for a message to be shown. It's shown along with the message type. You will find the trigger event and message type in the MSH-9 part of the message.
For example, if you see ADT-A04 in the MSH-9 section, ADT is the message type and A04 is the Trigger Event. In the HL7 standard, ADT-A04 would signal the message of "patient register." There are a lot of different message formats to keep up on. You can see more examples here.
I'm not going to go into every single message type but here are some of the more commonly used ones:
ADT - Admit, Discharge, Transfer
ACK - General acknowledgment
BAR - Add or change the billing account
MDM - Medical document management
DFT - Detailed financial transaction
ORM - Order (for treatment or pharmacy)
MFN - Master Files Notification
QRY - Query, original mode
ORU - Observation results unsolicited
RAS - Pharmacy/treatment administration
RGV - Pharmacy/treatment give
RDE - Pharmacy/treatment encoded order
SIU - Scheduling information unsolicited
You can see the full list of HL7 message types here.
How are they transmitted?
Now that you know what some of the HL7 message types are, I'll explain how they're sent. First, you'll need to create a listener so you can receive the messages. This may sound complicated but it's just a TCP listener. Then you'll need to make another thread that sends HL7 messages or else the listener won't be able to get the messages. When your listener has received a message then it needs to send a message back. This is commonly referred to as an "acknowledgment."
Here are the steps you would go through to receive a message and send back an acknowledgment:
Create console application: File > New > Project. Choose the console app, give it a name like HL7 Listener then click OK.
Make a class for your messages: Make a new class and name it message or something similar.
Form a Segment class: Next, you need another class that contains the information of the segment. An easy way to do this is to create a new class and simply name it Segment.
Manipulate Your Segment Class: By adding fields, methods, and constructors, you can easily control your Segment. This is something you can do by holding the fields by utilizing a dictionary object. The fields use a certain type of message that have very specific locations in the segment.
Now you know what HL7 is, how to read the codes, and how they're transmitted. But how does all of that improve interoperability? In order for modern health care to be effective and efficient, information needs to be shared with other health care providers. This has been a problem in the health care industry for a long time. Accountable Care Organizations work mainly to improve communication between providers and EHRs play a huge part in this as well.
Legacy Systems
Legacy systems have their networks hidden behind closed walls. If you work in a legacy situation, this makes it incredibly difficult to share information. In the past, legacy organizations had to put information into a text file and try to safely send it to another organization. So, if you have a legacy system, you need to have file formats to write health data on and use your EHR to exchange the data with other health care providers. All of this had and has to be agreed upon with the other organization.
With HL7's universally agreed-upon messaging standards, it's much easier for you to group that information in a file and securely send it to the organization you need to communicate with.
Online Systems
Online systems are essentially constructed the opposite of legacy systems. For example, internet systems are built to be open and shared easily, and because of that, the information they share needs to be secure when it's exchanged. Online health systems are growing and will continue to grow. And while online-based systems don't use legacy or HL7, they need to be able to send and receive HL7 documents and messages for backwards compatibility with legacy systems.
In short, HL7 improves your interoperability by making it easier for legacy systems to securely share medical information while also making web-based systems compatible with legacy.
How to learn HL7
If you're looking to learn HL7, HL7.org has various 12-week courses throughout the year you can register for. The courses are designed for people that are novices at HL7 and help you learn through hands-on guided exercises. Oh, and it's a self-paced course allowing you to learn at your own speed.
Once you've finished the course, you will know how to do the following:
Read and understand the most commonly used HL7 standards
Understand HL7's controlled vocabulary
Know when to use messages and documents
Handle projects with interoperability problems across different health care systems and more
HL7 Summary
HL7 is a set of standards and definitions used across the globe to exchange medical information between medical care providers, commonly used in EHRs. There are seven different types of standards. The message types are based on a series of letters and numbers that indicate various actions such as admitting or discharging patients. You can take a course online to help you learn how to understand and use HL7 codes.
If you're in need of a behavioral health EHR, we offer the best software on the market! You can schedule a free demo here.
What is an ACO? How does an ACO work? Workers in the health care industry need to know about ACOs. ACO stands for Accountable Care Organization and they're comprised of groups of doctors, hospitals, and other providers of health care. These medical professionals voluntarily coordinate with each other to provide quality health care to patients on Medicare, Medicaid, and commercial insurance according to CMS.gov.
Do you think ACOs are working? Comment below with "yes" if you believe they are or "no" if you don't think they are. I'm curious to know what your thoughts are on the subject.
If you're a medical provider, you would do this to help your patients get the right care at the best time. Doing this can also help you steer clear of providing services your patients have already received which can consequently prevent other health care errors. When ACOs work effectively in providing good care and while cutting spending, they share the savings.
You can see the obvious benefits of participating in an ACO, which is why the Affordable Care Act (ACA) incentivized this for health care providers. Since 2011, approximately 6 million Medicare beneficiaries have joined an ACO. Combine that with the private sector, a minimum of 744 various health care providers have become ACOs themselves, according to Health Affairs in 2015. As of that date, about 23.5 million Americans were being served by ACO.
https://youtu.be/3rs8kpoXmWw
How does an ACO work?
Now that you know what an ACO is, you also need to know how an ACO works. When the ACA passed into law, it created the Medicare Shared Savings Program. ACOs then provide financial incentives for medical professionals who provide good care. But, ACOs only work if you and the other participating providers do a good job of sharing patient information.
It should be noted that you have to share patient information in a way that doesn't violate HIPAA. You can learn more about how to avoid HIPAA violations here. Under the ACA, every participating ACO must manage the health care for at least 5,000 patients on Medicare for a minimum of three years.
ACOs that provide high-quality health care while also saving money (and that should happen if you're sharing information well) get to keep a chunk of the money they saved. When entering an ACO program, you have a couple of options to choose from:
Aim for a bigger return at the risk of losing money if you don't meet certain standards
Get a lower, more attainable goal with no risk of losing money
ACOs and HIT
With one of the main goals of ACOs being to cut costs, you can use meaningful use in Health Information Technology (HIT) to improve patients' self-care. HIT tools, such as Electronic Health Records (EHR) make your patients' information more available to health care providers. This also makes it easier for physicians to communicate patient information so the patient doesn't have to.
ACOs can also use patient-facing tools referred to as "patient portals." These allow patients to see their medical information that has been recorded in the EHR. This way, your patients can check their test results, get educational self-care materials, and more. You can learn more about the features and benefits of our EHR here.
Are ACOs only for Medicare?
This is a common question and the answer is no. ACOs work with Medicare, Medicaid, and private insurance companies. However, there are three different plans in Medicare ACOs.
Pioneer
Medicare Shared Savings Program
Next Generation
While the Next Generation model is similar to the Pioneer model, patients will have different experiences depending on which model they participate in. When health care providers save money in Medicare they get to keep a portion of those savings.
Medicaid ACOs
Medicaid ACOs differ from state to state as their approaches are designed at the state level. Some Medicaid ACOs are similar to Medicare ACOs while others follow a more traditional Medicaid managed-care structure.
Some states that currently have Medicaid ACO plans include Utah, Colorado, Oregon, Illinois, Minnesota, Vermont, Arkansas, New Jersey, Maine, and Iowa. Other states have announced coming out with Medicaid ACO models.
Commercial ACOs
Commercial ACOs have the most variety of all ACOs. People with private health insurance that is part of an ACO should see a drop in the amount they pay for premiums and out-of-pocket costs. This decrease most likely won't be seen immediately. It should also be noted that consumers could see a rise in costs depending on if their provider requires preventative health care or disease management programs.
If you're enrolled in a private ACO, you might also have a change in your network provider. This is because some plans have very specific provider network providers.
What are ACO quality measures?
CMS.gov established ACO quality measures for 2018 and 2019 to make it easier for you and other medical providers to understand. Quality performance measures or benchmarks are certain performance standards an ACO must hit in order to earn points for that specific measure.
The system starts with the 30th percentile and ends at the 90th percentile. In the Shared Savings Program regulations, you will encounter circumstances where the benchmarks are flat percentages. These flat percentages are used to help your ACO get high scores. Once your ACO has a high score, it can earn the max amount of points.
You can see all the points scoring system and quality measures here. Keep in mind that all your "pay-for-reporting" needs to be 100% complete and as accurate as possible.
Are ACOs working?
The results have been mixed.
The purpose of the ACA in 2010 was to stop health care costs from continuing to skyrocket. ACOs are an important part of this. However, ACOs had not saved the government money, according to a report in 2015, five years after the ACA was passed into law. The 333 ACOs in the Shared Savings program and 20 in the Pioneer program reported huge savings of $411 million. However, that was before they took into account paying bonuses. Including bonuses, these ACOs actually had a net loss to the Medicare trust fund of $2.6 million.
However, the Pioneer program in Medicare ACOs did save some money for CMS as it cut spending by 1.2%, according to the New England Journal of Medicine.
Today, many believe ACOs are working very effectively, and some definitely are. That being said, there are a lot of people out there who believe ACOs are just a temporary fix until we can find a more permanent solution.
ACO problems
In order for ACOs to work, they had to make some big changes that required big investments in order to share data seamlessly. These changes frequently included new care coordination and care management systems, and those aren't cheap.
Needing such large investments in the beginning stages meant you could only join an ACO if you had lots of money to begin with. So, once you met Medicare's standards, you could still very well be in financial trouble, according to Kaiser Health News. In fact, you can actually be worse off financially.
What if an ACO doesn't save money?
You've most likely heard the saying, "it takes money to make money." With ACOs, it takes money to save money. But what if your ACO invests money with the hope of improving care and saving money but they don't actually save money? What if you hire more nurse managers or invest in some other type of new care management system that doesn't end up saving you money?
Unfortunately, you might have to eat those costs. And, if you don't meet the quality care and savings standards of the higher-risk option, you may have to pay a penalty.
Fortunately, if your ACO is sponsored by a rural provider, you can apply to obtain payments in advance for the purpose of building the necessary infrastructure to create a high-performance ACO.
If you're going to get in the ACO game, it's imperative you make it work. Below are some tips I've included on how high-performing ACOs achieved success.
How successful ACOs work
We've established that there can be some problems with ACOs. But, some are extremely profitable and work really well. Here are some takeaways from successful ACOs:
The longer ACOs are in the program, the better they tend to fare. Any time you participate in a new program, it will take some time to understand how to navigate it and make it work for you. This is no different here
Physician-led ACOs typically outperform hospital-ed ACOs. The reason for this is that bigger companies are more likely to have business incentives that conflict with the program
Reducing high-skill nursing and in-patient hospital services while continuing with high primary care use has been one of the key factors for ACOs to get good results. ACOs that have shifted focus in these areas have surpassed others in improving quality health care and reducing costs.
But there's more to it than that. Health Affairs interviewed 11 of the 21 most successful ACOs in 2018 to see what made them the best. They found that the highest achieving ACOs had these three things in common:
Worked to have a "high-value" culture
Developed population health management programs
Came up with a process of accountability to make sure performance continues to trend up over time.
Be Innovative with population health management
One of the first things ACOs do is aim to better manage patients that are chronically sick and high cost. Successful ACOs did this. And if you're new to the ACO game, I strongly recommend this as a first step. High-performing ACOs have tried testing different strategies for their staffing models. Some tried placing care managers in community health centers to focus on face-to-face patient management. Others centralized their staff to emphasize telephonic care coordination.
This resulted in many care managers thinking outside the box to improve patients' self care. Some ACOs put procedures in place to educate patients to know the difference in something that can be managed at home vs a situation that requires a hospital visit.
One of the keys to having a successful ACO is being innovative and thinking outside the box. Focus on what you can do to provide better care for patients and help them avoid unnecessary hospital visits and costs.
How do ACOs affect patients?
The goal of an ACO is to provide better care for Medicare patients while curbing rising health care costs. So with the goal of providing better, higher quality, more timely, well-coordinated, patient-centered care comes change in how that care is received.
A common issue for medical patients today is getting uncoordinated treatment. If you're the patient, you already have to schedule the appointments, potentially share test results with your clinicians, and get them to communicate with each other, not to mention deciphering through the various recommendations doctors give you. That's a lot to ask of someone looking for treatment.
The whole point of an ACO is to fix this problem, according to National Partnership. When done properly, your primary care doctor will communicate with the other medical professionals you need to be in contact with. A lot of ACOs actually have personnel that work specifically on coordinating care. This makes things so much easier for the patient.
ACO benefits for patients
There are a lot of benefits for patients in ACOs
Patients don't have to coordinate visits between doctors
Clinicians communicate with each other so patients don't have to share information
Educated patients spend less time and money on hospital visits with better self-care
Doctors recommend health care specialists for patients to see although patients are still allowed to choose a doctor that's not in their ACO
The downfall here is that many patients, if not most, don't know their provider is part of an ACO. However, an easy way to find out if you're part of an ACO is to simply ask your doctor.
Summary
What is an ACO and how does an ACO work? ACOs are Accountable Care Organizations that consist of doctors, insurance providers and hospitals with the purpose of providing better health care to patients through communication and coordination while saving the health care provider money. If those tasks are accomplished, the government will dole out bonuses to the ACO.
In order to have a successful ACO, you have to do a good job of sharing and coordinating patient information. While not all ACOs save money, the most successful ACOs focus on being innovative.
If you're a health care provider, having a really good EHR can help you achieve these goals in your ACO. Click here to schedule a free demo of our mental health EHR or simply fill out the form below.
What is Meaningful Use? It's a program enacted by the US Federal Government in 2009 to incentivize eligible medical professionals with payments to use a certified electronic health record (EHR), according to HealthIT.gov. The Meaningful Use program was designed to improve health care for patients by making it safer and more efficient. It's separated into three stages that we'll go over in a bit.
How does a clinic or clinician qualify for Meaningful Use? In order to become eligible, you need to show that you are meaningfully using it to improve the care your patients receive. Your hospital has to show the Centers for Medicare & Medicaid Services (CMS) that it has adopted, upgraded, and implemented certified EHR technology.
Participation in the Meaningful Use program comes with definite financial incentives. If you're looking for a certified EHR, you can learn more about how to choose an EHR here.
How does Meaningful Use improve quality of care?
The program is dependent on five priorities of health care policy, according to the CDC including:
Reducing health care disparity by improving efficiency, safety, and quality
Engaging with patients and their families in their health care
Your health care facility can get a lot of money for working toward these goals through an EHR. In fact, incentive payments start at $44,000 over a five-year period for Medicare Providers. Medicaid providers can get $63,750 in incentives over a six-year period. Those amounts are nothing to scoff at. However, keep in mind that these amounts depend on when a facility starts meeting the requirements.
Participation in the program started out as voluntary but that has since changed. It started out by simply giving incentives to physicians that participated. Now, providers who don't participate will be penalized with reduced Medicare reimbursements. So, not only does it pay to get in on the Meaningful Use program, but it also hurts you if you don't.
A really good EHR will also help you avoid HIPAA violations. And those can cost up you up to $5k per violation depending on the state you're in. All the more reason to have a really good EHR.
How many Meaningful Use stages are there?
There are three stages to this program and the stages build on each other over time.
Stage 1
Stage 1, launched in 2011, focuses on proper electronic data sharing through an EHR. The criteria for stage 1 consists of 15 core requirements and 10 menu requirements. Providers must meet all of the core requirements but only five of the menu requirements are needed to complete this stage.
If you want to get 100% of the incentive, you have to meet the standards of meaningful use for a minimum of 90 days.
Stage 2
The emphasis here is on properly exchanging patient information and care coordination. In order to meet the requirements for stage 2, you must continue meeting the requirements of stage 1. Stage 2 launched in 2014 and requires health care professionals to reach a larger number of their patient populations through their EHR.
To qualify for payment in stage 2, Eligible Professionals (EPs) need to qualify for 17 core objectives and 3 out of 6 menu objectives. Eligible Hospitals (EHs) and Critical Access Hospitals (CAHs) need to qualify for 16 core objectives and 3 out of 6 menu objectives.
One of the core requirements for EPs is to have the capability to submit electronic data for immunizations. For EHs, one of their core objectives is to be able to submit electronic data for immunizations, Reportable Laboratory Results, and Syndromic Surveillance.
Stage 3
The third and final stage of Meaningful Use is all about improving patient outcomes. But remember, you have to continue stages 1 and 2 in order to receive payment for stage 3.
Stage 3 has eight required objectives for clinicians to meet in order to avoid penalties and receive incentives. The eight objectives are as follows:
Protected Health Information: Also known as PHI, physicians have to conduct a "security risk analysis" to prevent patient PHI data leaks. This is also a HIPAA requirement, which, if violated, can result in huge fines
Electronic Prescribing: You need to send at least 80% of your permissible prescriptions to pharmacies electronically
Clinical Decision Support (CDS): This is a two-part objective. The first requires implementing five CDS interventions and the second requires active checks on drug and drug-allergy interaction
Computerized Provider Order Entry: EPs need to meet the following three standards: medication, lab, and diagnostic imaging orders
Patient Engagement: At least 80% of patients need to be able to view and download their health records through your EHR. You must also provide educational information to at least 35% of your patients
Coordination of Care: This is meant to increase patient engagement through three processes. 1) Have at least 25% of patients use your EHR. 2) A minimum of 35% of your patients must obtain secure digital information from a health care provider. 3) You need to get data from a minimum of 15% of patients through fitness trackers/wearable devices. EPs need to shoot for all three standards but only meet the requirements for two
Health Information Exchange: The focus here is twofold. 1) At least 50% of care record-transition must be done electronically. 2) When seeing a patient for the first time, you must receive health records electronically no less than 40% of the time
Public Health Data Reporting: Here, you need to choose three of five EHR destinations to submit data. The options include a public health registry, clinical data registry, syndromic surveillance, cases, and an immunization registry.
MACRA and Meaningful Use
What is MACRA?
The Medicare Access and CHIP Reauthorization Act, or MACRA, gives EPs and EHs more tools to provide patients with better care. MACRA created the Quality Payment Program (QPP), which is designed to benefit providers that provide great health care. QPP gives you various payment options as well.
The QPP is designed to do the following according to CMS.gov:
Repeals Sustainable Growth Rate formula. This was predicted to make cuts of 25-30% each year for the services you and other clinicians make to Medicare beneficiaries
Gives bonus payments to participating providers with alternative payment models (APMs)
Makes multiple quality programs faster and more efficient under the new Merit-Based Incentive Payments System (MIPS)
Requires all Social Security Numbers be removed from Medicare cards by April 2019
Changes how clinicians are rewarded for value and volume by Medicare
You can participate based on the following factors:
Size of your practice
Specialty
Patient population
Specialty
In short, MACRA created a way for health care providers to be paid for Medicare beneficiaries. It also set rules for data sharing.
What are MACRA's data sharing rules?
The CMS's Qualified Entity (QE) program helps your organization get Medicare claims data and this can be used to determine the performance of the provider. If your organization is or has been approved as a QE then you're required to produce and publically provide reports approved by the CMS.
QEs are also allowed to make non-public analyses and sell it to users that have been authorized, and you're also allowed to give out or sell combined data/information, including Medicare data at no cost to authorized users. The CMS certifies and monitors QEs that receive this data. You can see which QEs the CMS has certified, the region they're in, and the date of certification here.
How Meaningful Use and MACRA work together
When MACRA came out, Meaningful Use turned into part of MIPS, another part of MACRA. If you're a clinician, you won't participate in the Meaningful Use program for Medicare Eligible Professionals. Instead, QPP has incentives for clinicians to use certified EHR technology and includes categories based on performance like Advancing Care Information and Quality Measures Reporting in MIPS.
MACRA's new payment system aims to make it easier for your organization to simplify payment models and value-based health care delivery. Starting in 2019, if you treat Medicare patients, you will most-likely have to choose between using MIPS or APMs as your payment track. I say "most likely" because not clinicians will have to choose between these two tracks.
Under the new rule, you will get reimbursed based on a performance score on the following four factors:
Quality measures (30%)
Resource use (30%)
Meaningful Use (25%)
Clinical practice improvement activities (15%)
MACRA provides a path for you and your clinic, if eligible, to receive reimbursements through APMs or MIPS. But this isn't all new. Health care providers have been reporting on quality measures for a long time now under different programs, including Meaningful Use, Physician Quality Reporting System, Value-Based Payment Modifier program, and e-prescribing.
Are MACRA and Meaningful Use good for health care providers?
There have been a lot of reactions to MACRA and Meaningful Use, as is the case with any government regulation. Some health care professionals and clinics have lost money as a result while others have seen significant gains.
But are these programs good for health care? I believe they are. Obviously, I'm a huge fan of doing things that help hospitals be more efficient and help more people get treatment. I strongly believe that a great way to improve health care and get people the treatment they need is through having a really good EHR.
While I believe EHRs are a great way to improve health care, I also strongly believe that you have to use the EHR that's right for you and you need buy-in from everyone who will be working with it. If you're looking for a substance abuse or mental health EHR, you can also get a free demo of ours here.
How has Meaningful Use affected you?
We want to know what your thoughts are on the effects of Meaningful Use. Has it been positive or negative? If you think it's been good, comment with the word "good" below. If you think it's been bad, comment with the word "bad" below. I'm just curious about how many of you approve or disapprove of it.
Conclusion
In conclusion, Meaningful Use is a program created by the Federal Government with the purpose of incentivizing clinicians and health care providers to improve health care by using a certified EHR. It has three stages, each of which builds upon the previous stage. and has seen some significant changes since its inception in 2009.
Even if hospitals and clinicians weren't incentivized by the government to use an EHR, I'd still strongly recommend using one as I've seen providers increase their revenue by as much as 30% after switching from a paper to a digital EHR.
Which is the best treatment for drug addiction? In-patient or outpatient rehab, or detox? Sadly, many people have to ask these questions in order to help themselves or loved ones. The best drug addiction treatments include behavioral and medical health services tailored to the patient's needs and prevent relapse in the long run. In short, the best treatments are specific to the challenges of each individual patient.
There are many different treatments out there to help patients struggling with drug addiction. Some of those include:
Medication
Counseling
Treatment for other co-existing mental-health struggles like anxiety
Withdrawal treatment medical devices and applications
Preventing relapse in the long-term
Using Technology For Long-Term Recovery
The ideal treatment includes a mix of each item listed above. However, one of the most important steps in this process is giving patients the tools to stay off drugs in the long-term and prevent a relapse.
When patients get treated for addiction, they need to have communication with their therapist through technology. Therapists can send surveys to patients to see how they're doing and what help they need at that time. This helps the patient and the clinician.
Inpatient, Outpatient or Detox? Which Is The Best Treatment For Drug Addiction?
It's hard to know which drug treatment is best. To help, I'll break down what each one is and its benefits.
Inpatient Rehab Treatment
This is when a patient temporarily lives in a rehab facility. Inpatient treatment can be ideal for people with severe addictions, those who lack a solid support system, and people who have mental struggles like anxiety or depression. They usually offer individual and group therapy. Patients who have relapsed in the past may want to consider inpatient treatment.
Outpatient Rehab Treatment
Not all people need inpatient therapy. It's actually better for some people to start in outpatient therapy. That being said, outpatient treatment can also be a second step for people who have completed inpatient therapy. Outpatient treatment doesn't provide around-the-clock care but the treatments should still last at least 90 days. Anything less than that and the program isn't likely to be effective.
Detox Programs
Detox programs are good because they help people get drugs out of their systems safely. They're a good first step for people with moderate to severe drug addictions. These programs can be especially useful for people with severe withdrawal symptoms. By using medication, they can taper down a patient's usage until his/her body can handle not having drugs in it.
Are Drug Treatment Programs Successful?
The answer to this question is yes, they can be very successful. According to research by the National Institute on Drug Abuse, most people who get treatment are able to overcome drug addiction and become contributing members of society again. I should mention that a person's success in overcoming addiction depends on several factors:
Severity of the addiction
Cause and underlying problems
Getting treatment specific to the addiction
Quality of interaction between the patient and the providers
Principles Of An Effective Drug Treatment
Whether you're a medical practitioner looking to prescribe specific treatment for someone or a patient trying to figure out which is the best treatment for drug addiction, there are principles to consider. Here's a list of effective drug-treatment principles from the National Institute on Drug Abuse:
No treatment is right for everyone: The treatment needs to match the addiction to help that specific individual be a fully-functioning member of society.
It needs to be very accessible: Overcoming addiction is hard. That's why the barrier to entry needs to be very easy. They need to be able to get treatment the moment they're ready.
Addiction affects brain function and behavior: Using drugs changes your brain's function. This is part of why people frequently relapse down the road. This is one of the reasons patients need to have good communication with their therapists through technology.
Get treated for the right amount of time: The right treatment will be based on the severity of the addiction. Most people need at least three months of treatment in order to overcome their addiction, according to research.
Focus on more than just the addiction: Rarely is it just about drugs. The right treatment will focus on problems dealing with work, the law, health, and the patient's psychology, as well as the addiction.
What Makes A Good Drug And Alcohol Treatment Center?
Now that you know how to find which drug treatment is best, you might wonder what makes a good drug and alcohol treatment center? Just as no treatment is right for everyone, the same is true of treatment centers. There isn't one treatment center that fits the needs of every person battling drug addiction.
Different treatment centers have different specialties. Whether the center has a lot of specialities or only a few, what matters most is if they specialize in the treatment you require. Look for a center that's highly-rated and well-respected for the treatment you need.
Is The Staff Accredited?
You know who deals with patients the most? The center's staff. That's why it's really important to make sure they're accredited and dedicated. The best way to figure this out is to ask questions. Is everyone on staff a registered nurse? How many physicians work at the center? How involved are they in the treatment? Don't assume that just because they're accredited that it's a great treatment center. That's not always the case. But it is a good indicator.
Do They Focus On Underlying Problems?
As I mentioned earlier, the problem is rarely, if ever, just the drugs or alcohol. So, getting treatment only for those issues, without focusing on the underlying cause, won't result in lasting change. The best treatment centers focus on fixing the underlying problem that's causing the addiction.
Do They Offer Multiple Types Of Therapy?
People looking to overcome drug abuse should get several different types of therapy. Different therapies help because they look at the problem from different angles. Group therapy is excellent and helps a lot of people. And 1-on-1 therapy is just as important and effective. A treatment center that focuses on multiple kinds of therapy will be much more effective in helping people overcome addiction than those that don't.
What's Their Success Rate?
While there's no single factor that determines if a treatment center is good or not, this is probably the most important factor. For the most part, the best treatment centers have higher success rates.
But look deeper than the surface on this. How do they determine success? Is it based on the number of people who complete the program or former patients staying sober for x number of months? Also, keep in mind that some treatment specialties have lower success rates than others. So, that begs the question, how high is that treatment center's success rate in that specialty? How does it compare to other treatment centers with the same specialty?
Conclusion
So, which is the best treatment for drug addiction? It really depends on the needs of the individual and the severity of their addiction. What's incredibly important is choosing the right treatment center.
Are drug treatment programs successful? They can be very successful! What's really important here is getting the person into a really good treatment facility. You can know if a drug treatment center is good by looking at their specialties, staff accreditations if they focus on underlying problems and focus on multiple types of therapy, and their success rate.
There's a common concern out there: Can you trust the information you find on the internet? And just as important, if not more so, is: "How much of healthcare information online is accurate?". Here, we'll dive into how to find accurate healthcare information online.
The short answer is: It depends. You can't trust all of the healthcare information you find online but some of it is definitely reliable. Let me explain.
1. Use trusted sites
When you're looking for healthcare information online, you'll probably start with a Google search. But you don't want to trust every website you find. Some of them will have outdated information.
A good way to know if a website is reliable is if it's sponsored by Federal Government agencies. To check for this, go to usa.gov. While that's a great resource to help you verify a medical website, it's not necessarily the first resource you should use. Here's a list of medical websites that are trustworthy:
MedlinePlus.gov: Not only does this website have a lot of useful and accurate healthcare information, but it also has an online tutorial on how to know if you can trust online healthcare information,
Smart Patients: This website was founded to help patients learn about medical developments dealing with their conditions and it does exactly that. Smart Patients has a built-in search engine that helps people find and track clinical trials of their choosing and discuss them on the website's forums,
Drugs.com: A huge part of healthcare is the medications you need to take. Drugs.com is fantastic because it gives you information about drugs, their uses, and how they might react to other medications. This site also has its own search engine to help you find legal drugs by their appearance or name. It should be noted that the search engine only pulls from the US,
National Health Information Center (NHIC): NHIC helps patients and medical professionals get in touch with organizations to get reliable answers to their healthcare questions. This site also keeps a calendar of days, weeks, and months with the purpose of helping people learn about various healthcare topics,
National Center for Complementary and Integrative Health: Like USA.gov, this website helps patients verify a medical website's reliability. It has a list of healthcare websites that are useful and also detailed guidelines on how to evaluate a medical website.
2. Check the healthcare information dates
If a website doesn't have current information, that's a huge red flag. When you're searching online, pay close attention to the date the information was written. If the information is older, it could still be relevant and accurate, but it could also be out of date. As a general rule of thumb, the most current medical information is generally the most trustworthy.
3. Ask yourself some questions
If you're using a website other than the ones mentioned above, ask yourself some questions.
Does it have .gov at the end of its URL? Another general rule of thumb, if the website ends with .gov, it's probably pretty reliable. This doesn't mean that websites ending in something else like .com or .org aren't reliable. But most government healthcare websites are solid sources of information. You can also check the site's "about us" section to see who runs it,
What's the purpose of the website? Is it selling you something? The websites we mentioned above are all there to solve a problem in the medical field and many of them are government-run. Look into the purpose of the website. If it seems sketchy or like the main purpose is to sell you something, then you should take it with a grain of salt,
Where does the website's medical information come from? Is it based on medical research or does it come from somewhere else? Does the website tell you where the information comes from? If the information is based on scientific research from a reputable source that's a great start,
Does the website promise the moon? Typically, if information seems too good to be true, it usually is. If they promise you a huge return with very little work or effort, then you should be very skeptical of that site,
Have experts reviewed the information? Quality medical information will have been reviewed by experts. Check the bottom of the page for the names fo medical experts who approve the information.
Is the site news or advertising?
Telling the difference between news and advertising websites can be hard. A lot of the time, advertising websites try to look like news websites to seem more credible. They'll even use logos from actual news sites.
Fake news or advertising websites tend to endorse certain products and even link to sales websites. News websites rarely do either of those things. If all of the comments are positive and you aren't able to comment, that's usually a sign it's a fake news/advertising website. News organizations almost always let you comment and they will usually have negative and positive comments.
Summary: How much of healthcare information online is accurate?
In summation, you should always be skeptical when looking for healthcare information and make sure you run what you find online by your doctor. Check to see what kind of institution runs the website and when it was last updated. And you should only trust information that's unbiased and based on scientific research.
One of the best ways to avoid websites with inaccurate information is to start with trusted websites. Use the websites we listed above to start your search. Run the website through usa.gov to see if it's run by the government.
Following these steps will help you find accurate healthcare information online. How much of healthcare information online is accurate? A lot. But there's also a lot of inaccurate healthcare information online. You just have to be careful about it.
Have you ever come across a healthcare website with information that just seemed too good to be true? Comment "yes" if you have and "no" if you haven't. I'm just curious how many of you have run into that and if it's been a frequent problem.
It's no secret that doctors know a lot. And sometimes, we think we know better. Sometimes we're right! But what are some things that doctors know, but most people don't? We want to look beyond the obvious stuff - beyond the fact that they know how to diagnose your sickness or how long it will take you to recover from an in-grown toenail surgery.
So, we created a list to answer the question, "what are some things that doctors know, but most people people don't". Here's a list of 14 things doctors know that most of us don't.
1. You Don't Have To Be Super Smart To Become A Surgeon
There's this belief out there that in order to work in the medical field in any way, you have to be brilliant. However, it just isn't true. Yes, there are many doctors out there who are incredibly smart and have a work ethic to match it, but they aren't all brainiacs. Sorry surgeons.
When it comes to surgeons, the average general physician tends to have more medical knowledge. Surgeons just tend to be better at what they get paid to do - surgery. And that's okay. They don't need to be amazing at everything medical. They just need to be good at what they do.
2. Not Everyone Who Went To Med School Can Prescribe Medication
The reality is that there are doctors who went to medical school who can't give you a prescription. There are lots of medical doctors who went to med school that can't prescribe medication. Pathologists and radiologists are a couple of examples.
3. Not All Doctors Can Read X-Rays
This is actually true of more than just X-rays. It also includes CT scans and MRIs. Frequently, when a patient asks a question about any of these, the doctor will often just read the report. Only the radiologist knows how to read your X-rays, MRIs, and CT scans. In fact, it takes a lot of experience to understand what's normal and abnormal in these images.
Have you ever had a doctor point out something in an X-ray and wondered how they were able to find that? I certainly have. Usually, the doctor showing it to you can't find it either - at least, not without help.
4. Stethoscopes Are Mostly Just To Hear Your Heartbeat
There are not a lot doctors can tell from just listening to your heartbeat. They can tell if it's irregular or regular and maybe a little more. But that's about it. There isn't a lot of diagnosing they can do just by listening. For instance, a doctor can't listen to your heartbeat and know that you need a triple bypass.
5. Doctors Don't Always Live Super Healthy Lives
They should know better, right? Anyone who knows a doctor closely can tell you that some doctors do things they shouldn't. A lot of doctors would admit this. There are doctors that smoke, eat way too much junk food, are overworked, and don't get enough sleep. This isn't to say that all doctors are this way. But hey, they aren't perfect.
6. They Aren't All Rich
Growing up, I thought that if you were a doctor then you must be rich - Filthy rich even! But doctors' salaries can be very deceptive. In fact, doctors actually make less per hour than teachers. That sounds outlandish but it's true.
When you consider the number of hours worked by both, the time spent in school and student loan debt acquired, doctors don't make as much as you think. You can read more about how doctors make less than teachers from Best Medical Degrees.
7. The Placebo Effect is a Real Thing
Even though doctors know this, they can't explain it. For some reason, believing that it will fix the ailment actually works. This isn't always completely cut-and-dry, but patients who believe the treatments their doctor prescribes for them tend to see more improvement to their ailment.
What is the Placebo effect?
The Placebo effect is when someone takes a pill or treatment and receives a positive effect that can't actually be attributed to the treatment. Its benefits are instead attributed alone to the patient's belief that obtaining this treatment will fix the problem. You can learn more about the Placebo effect here.
8. Most Disease Treatments Should Continue Beyond Symptom Relief
Treatment for diseases need to continue even after the symptoms have gone away. It happens all the time that a patient has a disease, gets treatment, the symptoms go away, and the disease isn't cured. While the symptoms may be gone, the disease usually isn't and needs more treatment. When the patient stops getting treatment, the disease will come back.
This is part of why it's so important for doctors to use an electronic health record (EHR) that keeps the patient's treatment going. You can learn more about what to look for in an EHR software here. Or you can get a free demo of our EHR software.
9. You Can't Use Electric Shock To Bring Everyone Back To Life
Don't be fooled by movies and TV shows. It is true that using electric shock can bring someone "back to life" but only in very specific situations. It only works in a specific type of heart arrhythmia. In other situations, this procedure can actually kill the patient.
10. They Know The Sex of Your Baby at 12 Weeks
Sometimes doctors know things before they tell you. Knowing the sex of your unborn baby is one of those times!
Doctors perform ultrasounds early in the pregnancy to check the baby's health. However, by the twelfth week, doctors can usually see the sex of the baby if it's in the right position. By week 13, they can usually tell with extreme accuracy, but it's against the law for them to tell you the sex of the baby that early.
11. Saying "I Don't Know" Can Be A Good Thing
If your doctor says "I don't know", that's a sign of honesty. No doctor is right all of the time and one that pretends to be is likely not always being honest with you. If a doctor is willing to be up front with you and ask other doctors for help, that's a great sign he's trustworthy.
12. Most Fevers Don't Need Antibiotics
Many illnesses don't get better with antibiotics. When it comes to fevers, antibiotics won't help the fever more quickly, most of the time. In fact, most fevers can't even be diagnosed early on. It's not that no treatment is required for most fevers, it's just that they don't need that specific kind of treatment.
13. Famous Doctors Aren't Always The Best
It's hard to know if a doctor is really a good doctor. Ratings and reviews don't always help because they can be heavily influenced by the nurses, wait time, etc. A bad outcome doesn't necessarily mean the doctor did anything wrong. Sometimes that's just the way things go. And being nice doesn't equal being a good doctor either.
One way to know how good a doctor is can be by asking other doctors that know him/her. Nothing is fool-proof, but asking people with first-hand knowledge of his/her expertise can be really helpful in finding an excellent doctor.
14. Vitamins Are Usually A Waste of Money
Why we do say "usually? Because they're useful if you have a deficiency of that particular vitamin. But, there's no need to take a bunch of different vitamins every day.
Conclusion: What are some things that doctors know, but most people don't?
So, what are some things that doctors know, but most people don't? They know so much that no list could capture everything. But we managed to get a lot of the insider information. Here’s a quick recap:
They aren't all rich
You don't have to be brilliant to be a doctor (but it helps)
They can't all prescribe medication
Not all doctors can read X-rays, CT scans, or MRIs
Stethoscopes can't usually result in a diagnosis
Doctors eat and do unhealthy things (they're human too)
A patient's belief in a treatment can help it be successful
Disease treatments should continue after symptom relief
Electric shock can only work in very specific situations
They usually know the sex of your baby at 12 or 13 weeks
A doctor who admits not knowing can be a good thing
Fame doesn't equal the best doctor
Most fevers don't require antibiotics
Vitamins are't usually worth the money
What do you think of our list of "what are some things that doctors know, but most people people don't"? Is there anything we didn't add to the list that we should have? If so, comment below and we'll get it added.
If you're looking for a new behavioral health or addiction recovery EHR, we'll give you a free demo of ours. Just fill out the form below to get one scheduled.








 (877) 425-5382
(877) 425-5382